Secondary Prevention of Cervical Cancer
Adenocarcinoma in situ (AIS)
Colposcopic diagnosis of AIS is a challenge.

The colposcopic diagnosis of AIS is difficult, and often the examiner must rely entirely on the opaque acetowhiteness of the columnar epithelium and/or an accentuated pattern of vascular markings. Colposcopic findings in a 25-year-old gravida 0. The patient was vaccinated against HPV with quadrivalent vaccine at 18 years of age. Her cervical smear was reported as class III-g. High risk HPV types 16 and 18 were detected. Colposcopic findings appear normal before the application of acetic acid.
A well demarcated acetowhite lesion is rare in AIS.

Following the application of 5% acetic acid, colposcopy shows an isolated, opaque acetowhite lesion at 12 o’clock in an atypical T-zone type 1, which is classified as grade 2 (major change) abnormal colposcopic finding.
AIS presents in a tree-like structure.
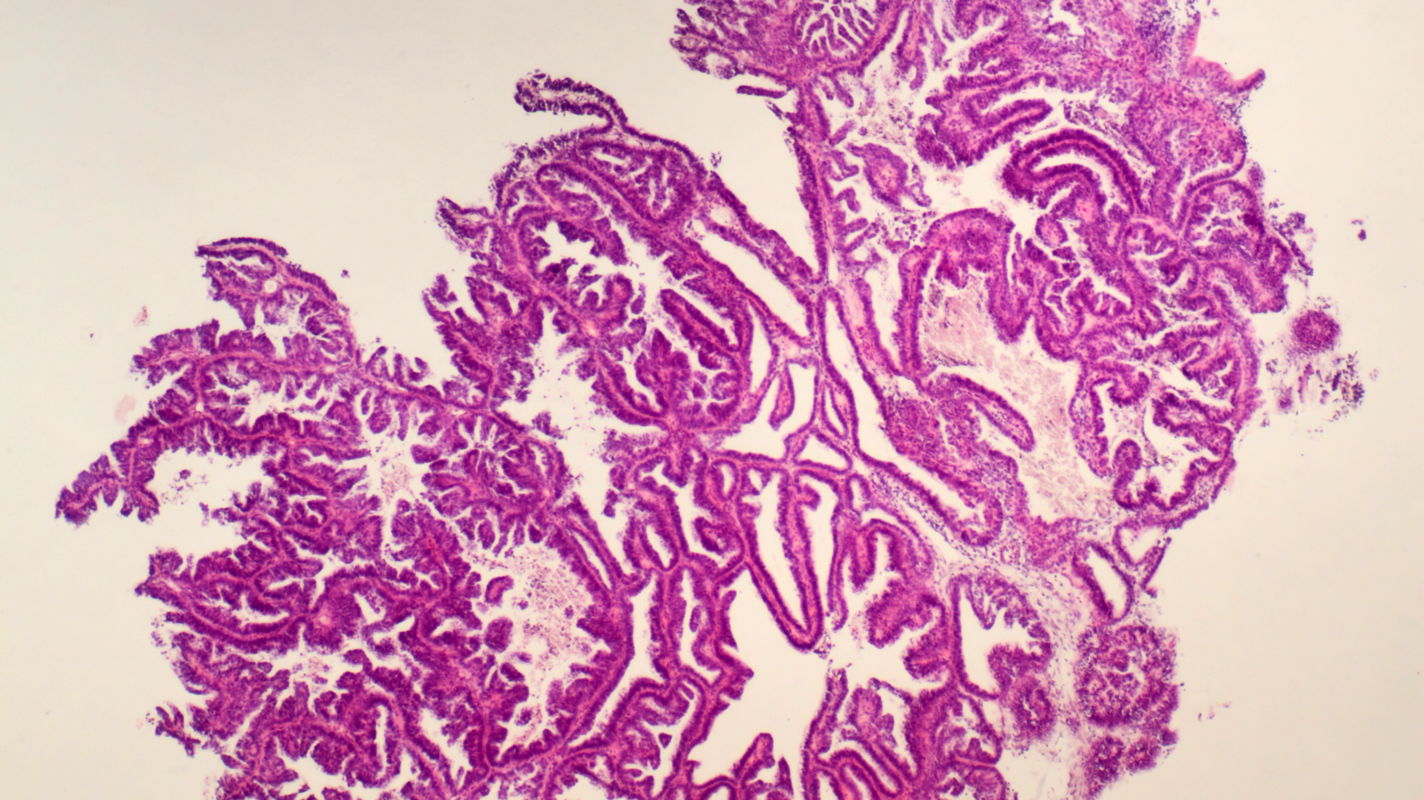
H&E stain of tissue sampled from the exophytic lesion at 12 o’clock by punch biopsy shows an arborizing pattern (‘tree’) of atypical glandular complexes. Polypoid exophytic growth is interpreted as endocervical AIS. The histopathologic diagnosis is adenocarcinoma in situ (AIS).
Diagnosis is made easier by immunohistochemistry.
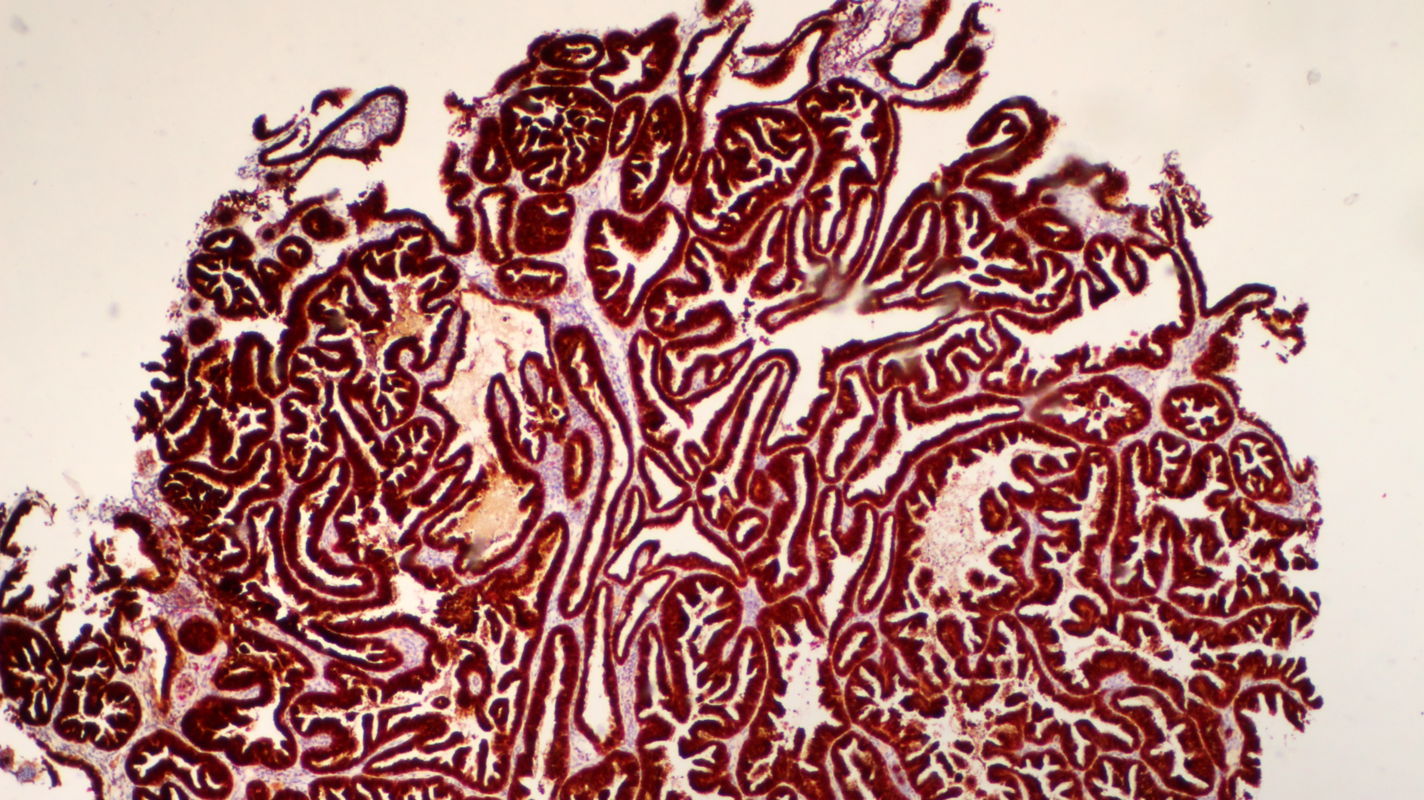
Detection of the immune markers Ki67 and p16 is strongly positive throughout the epithelium of the biopsy specimen.